

Key Takeaways on Split Billing
- Split billing separates Medicare, and some state Medicaid, claims for professional and technical charges on different forms and payment streams.
- For many rural health clinics (RHCs), split billing means UB-04 for professional services and CMS-1500 for certain technical/non-RHC services.
- Accuracy depends on clean documentation, correct coding/modifiers, and the right claim routing — small mistakes can trigger denials and rework.
- The fastest way to reduce errors is to use EHRs that support UB-04 and/or CMS-1500 and automate split rules.
For Medicare patient visits, medical billing staff sometimes need to submit separate claims for professional and technical charges to the Centers for Medicare & Medicaid Services (CMS) for reimbursement, even if the charges apply to a single visit. The same applies to some state Medicaid claims submitted to states. Billers have to use the right billing method to make sure services are billed correctly and comply with CMS or state guidelines. One submission method is Medicare split billing or split claim billing. Combined with accurate documentation and coding, split billing lets providers avoid delays or denials.
For timely reimbursements, providers and billing teams want to understand the different types of services covered, including preventive services and medical visits, and how to document and code split bills. They also want to understand which services need billed together versus separately, and which claim form (UB-04 or CMS-1500) to use.
This article focuses on split billing:
- What it is
- How to do it
- When it applies
- How to avoid common errors
- How to automate it
What Is Medicare Split Billing?
Split billing is just what it sounds like, splitting a visit or services across separate Medicare claims. In some cases, it’s splitting one claim across different claim components. It’s not splitting a patient invoice across payment methods.
Medicare claims can include different categories of charges:
- Professional charges, which cover the provider’s services or rural health clinic (RHC)-covered services billed to the RHC all-inclusive rate (AIR)
- Technical charges, which are the non-physician components of care, such as equipment, supplies, medications, nursing/support staff, and certain diagnostic services
- Institutional charges, which are billed by a hospital or provider-based clinic and include facility-related services like room use, staff, supplies, and technical components
- Non-RHC services, which are services not reimbursed under the RHC AIR.
A Medicare split billing claim is used for a visit that includes both professional and technical components that are billed separately. In RHCs), this happens when a qualifying visit is billed under the AIR and additional non-RHC services are billed separately. CMS and applicable states require certain technical charges and non-RHC services to be billed on separate claims because they’re reimbursed differently from the core visit. In these cases, a single patient encounter may have two or more related claims.
This is different from a split (or shared) visit, which refers to how evaluation and management (E/M) services are billed when more than one provider participates in a facility setting.
For split or shared E/M visits in a hospital or outpatient facility, if two providers are involved in one encounter, the provider who provides the largest part of a service (the substantive part per CMS) bills for it.
Split billing (or split claim billing) describes how charges are routed on claims and often covers professional vs technical charges or non-RHC services done on separate claims on separate forms or parts.
For non-RHC services, split/shared visits describe who bills for an E/M service based on the amount of time or MDM per CPT/CMS rules.
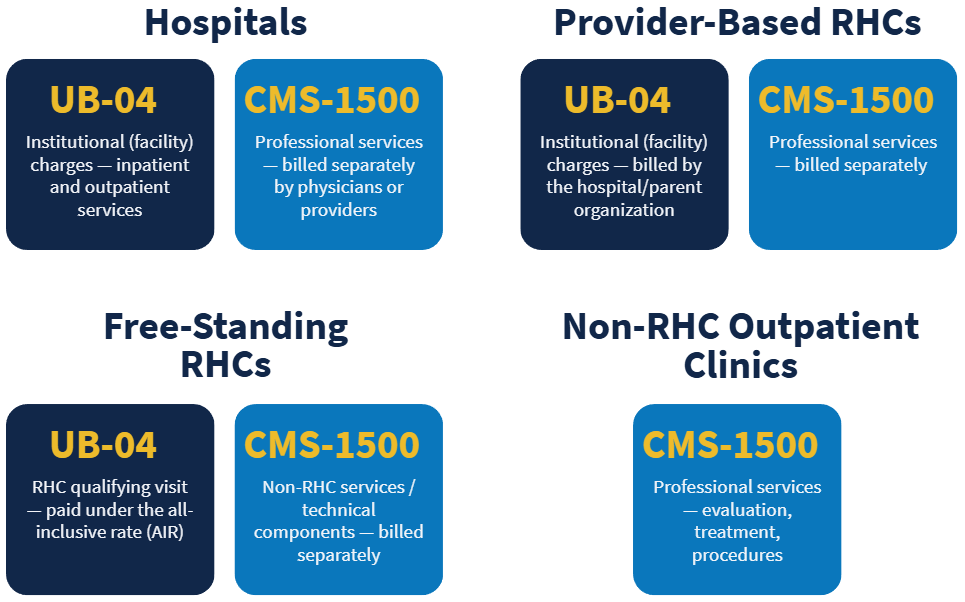
Providers have to follow billing and coding guidelines mandated by CMS (or states for Medicaid visits) when billing for shared services. CMS and applicable states accept split claims on two forms: UB-04 and CMS 1500. Typically:
- Hospitals and provider-based RHCs bill institutional (facility) charges on a UB-04 form (CMS-1450), while professional services are billed separately on a CMS-1500 form.
- Freestanding RHCs bill qualifying visit services under the RHC all-inclusive rate (AIR) on a UB-04 form.
- Freestanding RHCs bill technical charges or non-RHC services separately, typically on a CMS-1500 form.
- Non-RHC outpatient clinics bill professional services on a CMS-1500 form.
Learn how UB-04 software RCM integration with EHR billing makes split billing easier.
When Do You Use RHC Split Billing?
CMS keeps the Rural Health Clinic Qualifying Visit List (RHC QVL). It’s a list of frequently reported HCPCS codes that qualify as a face-to-face RHC visit. If a qualifying RHC visit paid under the AIR includes services not paid under the AIR, the services are typically billed separately on CMS 1500.
Non-RHC services not subject to the AIR model include:
- Lab services
- X-rays and EKGs — technical only
- Ambulance services
- Leg, arm, back and neck braces
- Prosthetic devices
- Hospice services related to a terminal illness
- Durable medical equipment (DME)
How Do You Bill Medicare Split Claims?
Billing for split claims requires understanding how to separate a claim (based on category of the components) and using the correct form. You also want to:
- Follow Medicare’s or your state’s Medicaid claim formatting requirements
- Make sure each claim has the right CPT/HCPCS codes, diagnosis codes, modifiers, and dates of service that apply specifically to that part of the claim
- Submit the claims individually and track their status through Medicare’s or your state’s Medicaid claims processing system to confirm payment or address a denial
Depending on your EHR and billing system, you may be able to generate both UB-04 and CMS-1500 claims, one of the two, or neither form in your EHR. Many systems are only designed for one claim type, which can lead to:
- Extra manual steps
- Disconnected tools/services
- Higher collection costs
- Delayed reimbursement or missed revenue
If your EHR only supports one form, to accomplish splitting a claim you may have to take multiple steps to clean up generated claims and rebill new claims.
Free Standing RHC Split Billing Example
If you see a patient for a Medicare annual wellness visit who has a new complaint, you might treat the problem-based issue in addition to providing preventive care. In this scenario, you need to clearly document the services as distinct. In RHCs, the qualifying visit is typically reimbursed under the all-inclusive rate (AIR), while certain additional services may be reported separately depending on CMS guidelines. When appropriate, the preventive service and the problem-based portion of the visit are billed separately with the proper documentation and modifiers.
Primary Care Practice Split Billing Example
You run a primary care practice and evaluate a Medicare patient for neck strain after a car accident. During the visit, you document the evaluation and management (for example, CPT 99213) and decide the patient needs a cervical collar (neck brace). Because the brace is durable medical equipment (DME), you bill Medicare for it separately from the office visit. You submit two separate claims: one for the professional medical service and one for the technical/DME supply item.
Hospital and Provider-Based RHC Split Claim Example
Hospitals bill institutional and professional services separately. For example, if a Medicare patient visits the ER, is placed in observation, and then admitted as an inpatient on the same day, the hospital submits one institutional claim for the outpatient observation and emergency services and a separate institutional claim for the inpatient admission and related care. Professional services are billed separately.
Split Billing Tips
When billing a split encounter for an outpatient visit, consider writing two separate encounter notes for each visit to make splitting the claim easier. Also ensure the billing team applies required modifiers and bundling rules, for example, CMS/NCCI guidance where applicable.
Note: Some Medicaid plans may require billing on two different claim formats depending on the payer/state and contract.
Coding and Documentation Requirements CMS Auditors Look For
Accurate coding and documentation are critical for split claim billing. Providers need to:
- Use standardized codes (CPT/HCPCS, ICD-10)
- Clearly document patient history, condition(s), and treatment plan(s), medical necessity, and services rendered
- Ensure separately billable services are supported by the record
- Keep documentation consistent with the claim route (UB-04 or CMS-1500)
The biller or billing service provider is responsible for ensuring documentation supports the codes and any separate charges get billed separately.
Common Mistakes to Avoid in Split Billing
To help reduce denials when doing split billing, avoid these frequent issues that can cause denials and rework:
- Using incorrect CPT/HCPCS codes or missing required modifiers
- Having incomplete documentation that doesn’t support separate claims or claim components
- Failing to submit required separate claims for non-RHC services
- Billing for services that aren’t covered or aren’t medically necessary
- Having your team not aligned on routing rules, such as who bills what, where, and why
Medicare Guidelines and Regulations 101
Another common mistake with split billing is not following CMS Medicare or state Medicaid billing process and guidelines. CMS and state guidelines specify how providers must code, document, and bill services, including:
- When to submit separate claims
- When to use modifiers
- Which services qualify for RHC reimbursement vs non-RHC billing
- Documentation expectations to support claims
Staying current with CMS and state updates and training your billing team reduces denials and compliance risk.
How Can You Maximize Reimbursements for Rural Health Clinics?
A Better Way to Do RHC Split-Claim Billing Is with Automation
Azalea created a workflow for automated split billing. As a result, splitting a claim with Azalea practice management software, ambulatory EHR, hospital EHR, or RCM billing services is easy. It applies a consistent set of rules — that you predefine — across encounters to empower you to automatically split claims and reduce coding errors, denials, and, rework.
The Azalea EHR also supports UB-04 software RCM integration and UB-04 and 1500 claim formats.
Does Your Billing Process Need a Refresh?
Speak with an expert to see what Azlea RCM billing experts and integrated EHR and billing software can do.


